Figure 1. Proportion of women receiving ARTs by birth cohort. Cohorts: 1962-1978
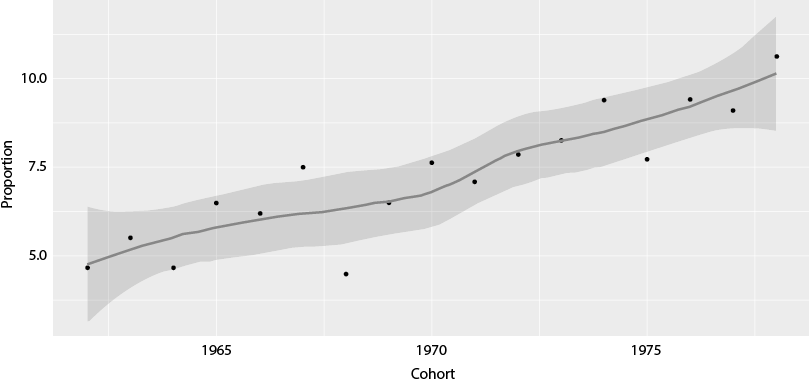
Source: Fertility Survey (2018).
doi:10.5477/cis/reis.194.103-120
A Study on Access to Assisted
Reproduction Treatment, Factors for Its Use
and Success Rates in Spain
Reproducción asistida en España: un estudio del acceso,
las razones y el éxito de los tratamientos
Mariona Lozano, Clara Cortina and Evgeniya Borisova
|
Key words Success
|
Abstract This article analyses the current use of medically assisted reproductive technologies in Spain and describes the profiles of women using them or wishing to use them. Data from the 2018 Fertility Survey and a simple probit regression model with instrumental variables were employed to examine the factors associated with the use and success of these treatments. Married women with higher socio-economic status and primary infertility are more likely to access them. Younger generations are resorting to them more often, possibly due to delayed childbearing, improved technologies, family changes and legal developments. The main barrier to accessing them is economic, which indicates that there is an unrealised potential use. Finally, when correcting for endogeneity, no statistical association was found between socio-demographic variables and the treatments’ success. |
|
Palabras clave Éxito
|
Resumen Este artículo analiza el uso actual a las técnicas de reproducción médicamente asistida en España y ofrece una descripción de los perfiles de mujeres que acceden o desean acceder a ellas. Usando datos de la Encuesta de Fecundidad de 2018 y un modelo de regresión probit simple con variables instrumentales, se examinan los factores asociados al uso y éxito de estos tratamientos. Las mujeres con mayor nivel socioeconómico, casadas y con infertilidad primaria tienen más probabilidades de acceder. Las generaciones jóvenes las usan más, posiblemente por el retraso a la maternidad, mejoras en las técnicas, cambios familiares y avances legales. La principal barrera para acceder es económica, lo que indica un uso potencial insatisfecho. Finalmente, al corregir la endogeneidad, no se encuentra asociación estadística entre variables sociodemográficas y el éxito del tratamiento. |
Citation
Lozano, Mariona; Cortina, Clara; Borisova, Evgeniya (2026). “A Study on Access to Assisted Reproduction Treatment, Factors for Its Use and Success Rates in Spain”. Revista Española de Investigaciones Sociológicas, 194: 103-120. (doi: 10.5477/cis/reis.194.103-120)
Mariona Lozano: Centro de Estudios Demográficos. CED-CERCA | mlozano@ced.uab.es
Clara Cortina: Universitat Pompeu Fabra | clara.cortina@upf.edu
Evgeniya Borisova: Universitat Autònoma de Barcelona | eborisova@ced.uab.cat
Introduction1
In Spain, as in other European countries, rising infertility rates and increasing difficulties in conceiving among couples who wish to have children are largely linked to longer life courses and the postponement of first childbirth (Rey, Grande and García-Gómez, 2022). Both phenomena are related to greater education levels among women, which entails, on the one hand, a temporary incompatibility between the role of mother and that of student and, on the other, higher professional aspirations (Martínez-Martínez and Bote, 2019). This leads to prioritising career development at an early age, consequently postponing both couple formation and the assumption of the economic, emotional and logistical cost of motherhood.
Spain, together with Italy, has the highest average age at first childbirth in Europe, at 31.6 years old in 2021, according to Eurostat data. The consequence of this delay is that many women begin their reproductive journeys at an age when natural conception is biologically more challenging.
According to an international study, the prevalence of infertility (defined as the inability to achieve a pregnancy after 12 months of regular unprotected sexual intercourse) is as high as 9 %, with 56 % of affected couples seeking medical treatment (Boivin et al., 2007). These figures are similar across both more and less developed countries and represent an increase compared to earlier estimates (Rochebrochard and Thonneau, 2005).
The use of assisted reproductive technologies (ARTs) has significantly increased worldwide in recent decades. While thirty years ago many infertile couples were unable to access medically assisted treatments (Olsen, Küppers-Chinnow and Spimelli, 1996), the current proliferation of specialised clinics and the partial inclusion of these treatments in public health systems have widened access. Assisted reproduction has become a key tool for reproductive endeavours, with important implications for the fertility levels of populations (Lazzari, Gray and Chambers, 2021).
The use of ARTs has been growing steadily in Spain. It is the European country with the highest percentage of births resulting from these treatments: 6.4 % in 2018 (Passet-Wittig and Bujard, 2021) and 8 % in 2019 (Devolder and Borisova, 2022). However, the available literature on their current use, related socio-economic inequalities and reasons for access or non-access remains scarce.
Previous studies have noted that the highest proportion of patients in treatment has been found between the ages of thirty-five and thirty-nine (63 %), in contrast to much lower proportions among women under thirty-five (10 %) and over forty-two (11 %) (Audibert and Glass, 2015). However, not all women can access these treatments with the same degree of ease. The most common barriers include financial cost, legal restrictions and socio-cultural factors. Studies have shown that women who conceive through ARTs generally belong to more advantaged socioeconomic groups, and possess higher levels of income and education (Harris et al., 2016; Goisis et al., 2020; Chambers et al., 2014; Alon and Pinilla, 2021). These women are also the ones who delay childbearing to the greatest extent and can best afford the cost of treatment.
It has also been suggested that the cultural acceptance of ARTs operates as a major driving factor for their use, even beyond differences in wealth, demographic structures or religious affiliation (Präg and Mills, 2017). Given the prevalence of delayed childbearing, the relative absence of legal barriers to assisted reproduction and the availability of public coverage for women below the age of 40, it is worth considering whether there is also socio-economic selection in access to ARTs in Spain.
Data from the 2018 Spanish Fertility Survey (Encuesta de Fecundidad Española de 2018) were analysed in this study to examine access to ARTs in Spain, as well as the factors that explain their rise. The following objectives were pursued:
In short, this article seeks to describe the current status of access to assisted reproduction technologies in Spain, as well as their degree of success. Although demand has risen markedly in recent years, suitable individual-level data to characterise both the women who reported needing these treatments and those who actually accessed them were not available until the publication of the 2018 Spanish Fertility Survey. The sample analysed consisted of 810 women who undertook treatment and 481 who would have liked to have had treatment. This allowed for a representative description, but it had limitations that preclude drawing generalisable inferential conclusions. This paper is therefore descriptive and points to potential avenues for future research that would make it possible to address this phenomenon more accurately and in greater depth.
Assisted reproduction treatments
In recent decades, the reproductive wishes and behaviour of Spanish women have changed significantly, and they are one of the main factors behind the low fertility levels observed. These changes include a preference for smaller nuclear families and a delay in the age of entry into motherhood. This delay is due to a number of factors, most notably including employment and salary conditions (especially among women), which extend beyond the early stages of the working career (Alcañiz and Monteiro, 2016; Baranda-Ortiz, 2019). Moreover, once a certain degree of job stability has been achieved, problems related to work and family balance also arise, which make it difficult for women to enter motherhood (Bueno, 2020). However, fertility desires remain relatively high in relation to actual fertility. While observed fertility is around 1.12 children per woman (INE data for 2024), desired fertility has been consistent at two children (Adserà and Lozano, 2021).
These structural factors are compounded by the biological constraints of delayed childbearing, which directly affect fertility, understood as the biological capacity to conceive. It is estimated that between 48 million couples and 186 million people worldwide live with some form of infertility (Passet-Wittig and Greil, 2021; Boivin et al., 2007). Infertility can be classified as primary (no previous pregnancies) or secondary (difficulty conceiving after a previous pregnancy). Given that measuring fertility poses significant methodological challenges, proxy indicators such as time to pregnancy or semen quality are often used.
Medically assisted reproductive technologies encompass a range of procedures that are generally divided into two categories: high-complexity procedures—such as in vitro fertilisation (IVF), embryo transfer and oocyte reception—and low-complexity procedures—including intrauterine insemination and programmed intercourse. The choice of procedure depends largely on medical considerations and takes into account factors such as the woman’s age, health and fertility. However, this study does not differentiate between the different modalities, but uses “assisted reproductive technologies” as a general, all-inclusive term, as the aim of the analysis is not clinical but demographic: to understand the profile of women who express the desire or feel the need to undergo these treatments.
The number of countries collecting and publishing systematic information on ARTs use has increased considerably in the last decades. In 2017, Europe was ranked as the region with the highest number of ARTs cycles performed (Zegers-Hochschild et al., 2017). Nevertheless, access to these treatments varies substantially between European countries: it is greater in the Nordic countries and in some western European countries, such as France and Spain.
Explanatory factors for differential access to ARTs
This section explores the factors that explain variations in the use of ARTs between different contexts. Comparing studies on the prevalence of ARTs use and medical care-seeking remains a methodological challenge due to differences in data quality and comparability, as well as to heterogeneity in measurement criteria (Fauser, 2019). However, the literature has identified several key factors that influence such variations.
One of the most relevant determinants is the economic cost of treatment. Affordability is a significant barrier to ARTs access, especially in countries with low public coverage, which leads to marked socio-economic inequalities (McCarthy-Keith et al., 2010). Even in contexts where these treatments are more widely available and employed, cost remains a critical factor. At the individual level, affordability (measured as the net cost of an ARTs cycle relative to average disposable income) is positively associated with higher utilisation rates. Whereas countries that provide coverage through insurance or public subsidies have higher levels of ARTs use, socio-economic barriers can still be found even in systems with widespread public funding (Goisis et al., 2020; Lazzari, Baffour and Chambers, 2022).
Social and cultural norms also play a key role. Factors such as normative age limits for childbearing, beliefs about the moral status of the embryo, individual reproductive rights and ethical considerations about different procedures affect the acceptance and use of ARTs (Billari et al., 2011; Präg and Mills, 2017). Religious beliefs have a considerable influence on the perception and acceptance of this technology as well, conditioning its use and legitimacy in different environments.
Demographic variables, especially the delay in age of entry into motherhood, are closely linked to an increase in the use of ARTs (Kocourkova, Burcin and Kucera, 2014). In societies where it is common to postpone motherhood, as is the case in Spain, these technologies are more often employed. Nevertheless, this association may be weakened when controlling for cultural variables and individual values (Präg and Mills, 2017). Fertility delay is also related to the increased use of specific procedures such as oocyte donation and reception (Passet-Wittig and Bujard, 2021).
In conclusion, understanding the factors that condition access to and use of ARTs is crucial in view of their growing relevance in contemporary reproductive dynamics. These treatments offer solutions to infertility problems and the risk of remaining childless, potentially contributing to mitigating the negative effects of delayed childbearing on total fertility (Sobotka et al., 2008). However, significant inequalities persist: ARTs use is more widespread among the better educated and wealthier, underscoring the need for policies that address access and affordability gaps (Goisis et al., 2024).
Previous studies on the Spanish case have shown the importance of economic factors in relation to assisted reproduction treatments. Romero Guadix et al. (2022) studied the correlation between the number of IVF cycles performed in the different autonomous communities and the GDP per capita of each region. They found an inverse relationship between the percentage of women accessing IVF and the level of economic hardship of the population. Martínez-Martínez and Bote (2019) also analysed the socio-demographic determinants of ARTs use based on data from the Spanish Fertility Society (Sociedad Española de Fertilidad) and found that educational level and female labour force participation correlated with ARTs use.
Spain currently has one of the most advanced and permissive assisted reproduction regulations worldwide (Melo-Martín, 2019). The first legal framework in this field was provided in 1988 under Law 35/1988, one of the first legal instruments to regulate assisted conception procedures in the world. Law 35/1988 incorporated key principles such as informed consent, risk disclosure, confidentiality of clinical data and minimisation of surplus embryos. It also allowed research on non-viable embryos and guaranteed access to ARTs for any woman (regardless of marital status) through the national health system, up to the age of 40.
The legislation was updated in 2003 by Law 45/2003 to reflect scientific and technological developments in the field. This amendment introduced limitations on the number of oocytes to be fertilised per cycle (maximum of three), allowed long-term storage of frozen embryos and regulated their eventual disposal. It also extended the legal framework for research on supernumerary embryos, without any restrictions related to the date of cryopreservation.
Law 14/2006 was enacted in 2006, repealing the prior legislation, and established a new regulatory framework aimed at facilitating access to ARTs for people with fertility problems. This Law provided procedures to prevent and treat genetic diseases, banned reproductive cloning and introduced stricter requirements on the use of gametes and embryos. It prohibited financial compensation for donors, except for expenses related to time, effort and inconvenience. It also created official registers of both assisted reproduction centres and donors.
One of the distinctive features of the Spanish case is the sustained growth of the private sector in fertility services. ARTs treatments are expensive and have uncertain clinical outcomes. In 2018, average success rates per cycle ranged from 8 % to 27 %, depending on the age of the patient, and reached approximately 37 % in cases with oocyte donation (Sociedad Española de Fertilidad, 2018).
Although the national health system offers free treatment, it generally does not include gamete donation, except in cases related to genetic diseases. The rationale for public funding of ARTs lies not only in the demographic implications of infertility, but also in its effects on mental health and well-being: many studies have associated infertility with symptoms of depression, anxiety and relationship strain (Dhalwani et al., 2013). Public coverage not only promotes equity in access, but also contributes to reducing the financial burden on young households (Chambers et al., 2014).
Currently, the Spanish public health system covers up to three ARTs cycles for childless couples, with an age limit of forty years old for women and fifty-five years old for men (Alon, Guimon and Urbanos-Garrido, 2019). However, waiting times in public clinics average more than a year, which can compromise the effectiveness of treatment and generate mistrust among patients (Castilla et al., 2009). In practice, about 75 % of ARTs cycles are performed in private clinics. Recent studies have suggested that long waiting lists in public health care may explain the lower outcomes compared to the private sector (Alon and Pinilla, 2021).
Finally, it is important to consider social attitudes towards ARTs. In Spain, there is widespread support for these technologies: 86 % of the population are in favour and only 3.8 % are against (Aurrekoetxea-Casaus, Ronda and Govillard, 2022). These figures, which vary by gender and specific type of procedure, are significantly higher than those recorded in countries such as France or Germany, and are more similar to those observed in Italy and Sweden (Fauser et al., 2019).
This study analysed data from the 2018 Spanish Fertility Survey. This is a cross-sectional survey that collects information on two separate samples of men and women aged eighteen to fifty-five in order to study reproductive trajectories and aspirations. The survey provided information on the use of medically assisted reproduction technologies for the first time. Data were used only for the female population (N=14 556), as the original sample of men was very limited (N=2169), especially when stratified by birth cohort, educational level and fertility intentions, as well as access to ARTs.
A descriptive analysis was carried out of the characteristics of the women who had received ARTs (N=810) and those who had not received ARTs despite having problems conceiving (N=481). Any significant differences between the two groups were measured by comparing means. Specifically, the study looked at the distribution of education level, level of religiosity, place of residence, marital status, type of union, parity, and individual and household income. Educational attainment was categorised into three groups: primary or lower, secondary and tertiary education. In addition, the following variables were used: 1) birth cohort, grouped into 1962-1965, 1966-1969, 1970-1974; 1975-1979, 1980-1984, 1985-2000; 2) religiosity: not religious, not at all or not very religious, and fairly or very religious; 3) parity: zero, when the woman had no children, and birth order for those who did; 4) marital status (whether the woman was married or not married); and 5) household income (joint income of the woman and her partner [if she had a partner]), which was then been divided between income below the full sample mean and income above the full sample mean. The average was 3899 euros per month. Individual income, however, was grouped by categories in the original sample, which was recoded into (a) less than 1000 euros per month and (b) more than 1000 euros per month.
Finally, a simple probit regression model was estimated to measure the association between women’s characteristics and treatment success, controlling for treatment conditions. The dependent variable was coded as 1 if the woman had a child as a result of the treatment and 0 otherwise. Of the total number of women who underwent ARTs (n=810), 510 women achieved a pregnancy and 443 gave birth to a child, which yielded a success rate of around 55 % of those who received ARTs. The analysis included the following variables: level of education (measured at the time of the survey), degree of religiosity, age at the start of treatment (under thirty, between thirty and thirty-nine and over forty), type of treatment (artificial insemination, IVF, and others, including programmed intercourse and surrogacy), ownership of the reproductive centre (Social Security, private clinic or both), level of financial burden experienced to cover the treatment (significant financial burden or financially viable/no financial burden) and years of treatment duration (less than one year, between one and three years, more than three years).
This final analysis posed a methodological problem, namely endogeneity, since the variables associated with a higher or lower probability of accessing ARTs also predicted treatment success or otherwise. In particular, women with higher levels of education were found to be the most likely to be able to gain access to ARTs and were also the most likely to be successful, as higher education is also associated with a healthier lifestyle (Goisis et al., 2024). The same is true for age, as the quality of cells and eggs decreases with age. Likewise, salary, measured in the study in terms of whether ARTs represented a high financial burden, correlated with both the likelihood of access and with success, as the latter may occur after several repeated cycles.
Instrumental variables were used in an attempt to correct for this endogeneity. Being in a relationship at the time of beginning treatment served as an instrument, as it was correlated with the probability of accessing ARTs but not with the probability of having a successful outcome. A two-stage least squares (2SLS) procedure was used to obtain the instrumental variable (IV), in which the endogenous variables were modelled with one or more IVs in the first stage. These must be correlated only with the exogenous variable (education, age and level of financial burden involved), but not with the outcome (success). In the second stage, the endogenous variables properly adjusted by the instrument could be introduced into the main model producing unbiased coefficients (Wooldridge, 2002).
The problem with instrumental variables is that they are designed to work with continuous variables, but they can present problems in the case of binary variables, as is the case here. However, Angrist (1991) and Angrist and Pischke (2009) suggested that treating binary variables as if they were continuous in regression models with IVs may be a good solution. Consequently, two different models are presented in the text: a simple probit regression to model success (without controlling for endogeneity) and a linear model with IVs controlling for endogeneity.
This section outlines the results of the analysis in relation to: 1) the increase in the use of ARTs by cohort; 2) the socio-demographic profiles of women who did or did not receive ARTs, despite having faced reproductive difficulties; 3) the main reasons reported by those who did not access ARTs or discontinued treatment without achieving pregnancy; and 4) the factors associated with treatment success.
As shown in Figure 1, the percentage of women using assisted reproduction increased from 4 % in cohorts born in the 1960s to 10 % in cohorts born in the late 1970s. This increase can be attributed both to the rise in infertility linked to the delay in the age of entry into motherhood, technological progress in the available procedures and the expansion of coverage by the public health system.
Table 1 shows the characteristics of women who used ARTs versus those who did not, despite having faced fertility problems.
Statistically significant differences were identified in variables such as educational level, marital status, individual income and parity. Among the women who had accessed ARTs, 45.6 % had a university education, 80.6 % were married and 50 % reported high individual income. In contrast, among those who did not undergo ARTs, 41.3 % had a university education, 55 % were married, 23.6 % were single without children and 12.7 % were living with a partner; only 33.5 % had an individual income of more than 1000 euros net per month. A large proportion of ARTs users had no previous children (84.4 %), which indicated that the treatments were mainly used for their transition to first motherhood.
No significant differences were found between ARTs users and non-users in variables such as religion, degree of religiosity, size of municipality and autonomous community of residence. A marginally significant difference was identified regarding employment status (p<0.10): women who had accessed ARTs had a higher proportion of stable employment (48.9 % vs. 35 %) and a lower proportion of unemployment (9 % vs. 15 %), as measured at the time of the survey.
To analyse unrealised potential use, Table 2 presents the reasons reported by women who did not undergo treatment, despite experiencing difficulty conceiving (N=481). The majority mentioned economic reasons (56 %) or health reasons (32 %), indicating that barriers to access were predominantly material rather than attitudinal.
Table 3 lists the reasons adduced by women who discontinued treatment after failing to achieve a pregnancy (N=283). The main reasons were health problems and the decision to adopt (both 24.7 %), followed by emotional exhaustion (24 %). Fifteen percent mentioned financial constraints and 10 % reported that public funding was interrupted. Overall, financial reasons accounted for 25 %, which underlined the role of financial barriers in treatment abandonment.
Regarding treatment success, Table 4 shows the results of the simple probit regression that measured the association between the characteristics of women who had access to ARTs and the birth of a child that resulted from these technologies. The results show that variables such as educational level and religiosity were not significantly associated with treatment success. In contrast, factors related to socio-economic status, age, clinic ownership and duration of treatment were significantly related to success. First, women who underwent treatment in private clinics or combined public and private centres had a higher probability of having a child after treatment (coef.=0.68; p-value=0.000) than those who underwent treatment in public centres only. In addition, those who reported that ARTs had represented a minor or no financial burden also had a higher probability of success than those who undertook a major financial burden to access ARTs, most likely because they were able to opt for private centres. Finally, those who received IVF had a higher probability of success (coeff.= 0.35; p-value=0.05) compared to artificial insemination treatments, and age at the time of treatment decreased the probability of success; the older the woman was, the lower the probability that she might achieve a pregnancy and the shorter the duration of treatments.
However, when controlling for endogeneity, none of these associations was statistically significant (see Table 5). This suggests that treatment success was determined by other biological—not socio-demographic—variables that cannot be controlled for in this study. The Kleibergen-Paap test (available for Stata version 17) was used to assess the weakness of the instrumental variable. Since 26.39 (see Table 5) exceeded 10 % of the maximum size of the IV (13.68), the chosen instrument was considered not to be weak within the model used (Stock and Yogo, 2005). Nevertheless, this did not mean that the instrumental variable used could account for the possible dual causality between success and the probability of accessing ARTs, as measured by the variables included in the present study.
The main objective of this article is to describe the socio-economic profile of women in Spain who received ARTs, as well as of those who expressed the need for such treatments but did not undertake them. Despite the limited sample size (N=810), this study provides a unique source of information as to the reasons and barriers reported by women in relation to accessing ARTs in Spain, as there are currently no other comparable databases to address this issue in detail.
Although the analysis is mainly descriptive, statistically significant differences have been identified between the profiles of women who accessed ARTs and those who, despite needing it, did not undertake the treatment. Therefore, this paper provides a current “snapshot” of the socio-economic situation of women who use these techniques, which contributes to filling a gap in the national literature on the subject.
In general terms, the results are consistent with previous studies on Spain (Romero Guadix et al., 2022; Martínez-Martínez and Bote, 2019). These studies identified economic hardship as a major obstacle to accessing ARTs and emphasised the role of women’s education level and labour force participation in the need to access ARTs due to delayed entry into motherhood. In particular, Martínez-Martínez and Bote (2019) highlighted the need to improve work-life balance policies in Spain. This study complements these results, as it helps to understand the differences between the profiles of those women who could access treatment and of those who could not. It collects individual-level data derived from the 2018 Fertility Survey, which asked women about their reasons for not accessing or not continuing treatments.
In the sample, 6.8 % of women reported that they had tried to conceive (whether successfully or unsuccessfully) and benefited from medical assistance to achieve a pregnancy. However, only 60 % of this group had effectively accessed ARTs. The main reason identified for lack of access was economic in nature, revealing a potential unrealised demand due to financial barriers. Consequently, part of the potential births through ARTs did not happen due to lack of resources, in line with previous findings in other European countries (Boivin et al., 2007).
As expected, the results show that women with lower educational attainment (primary or compulsory secondary education) have significantly lower access to ARTs, which confirms patterns observed in previous research. There is also an increased use of ARTs among younger generations, which may be explained by the delay in the age of entry into motherhood, improved technical efficacy of ARTs, changes in family patterns and regulatory developments.
Economic status has been identified as the main obstacle to accessing ARTs, especially among women of older generations, which could be linked to more restricted public coverage in the past. Nevertheless, cultural factors, such as social perception and acceptance of these treatments, may also play a role. The results suggest that there is no direct relationship between access to ARTs and public funding: while in theory all women under forty can access the public system, there are long waiting lists (Alon and Pinilla, 2021), which limit actual access. In practice, only those women with greater purchasing power can use private clinics. This potential use has been enabled by the increasing social acceptance of ARTs, a legislative framework in place since the advent of the 2006 law on assisted reproduction that guarantees universal access, and a broad treatment coverage provided by the public health system.
From a socio-demographic perspective, access to ARTs is more common among women who are married or cohabiting with their partner, suggesting that reproductive endeavours in Spain continue to be primarily pursued within stable relationships. Single women or women who are not cohabiting with their partner are less likely to use these technologies as a route to single motherhood. A complementary analysis using the same database revealed that there is no significant association between delay in couple formation and treatment being sought, which may reflect a downward adjustment in reproductive desires in adverse contexts (Suero, 2024).
Nevertheless, previous studies have indicated that there are also structural constraints on access to ARTs for single women and lesbians, especially in public service provision (López-Rodríguez, 2017). The laws regulating reproductive techniques affect not only institutions such as clinics, gamete banks and medical bodies, but they also have a direct impact on people with infertility and, in particular, women. However, these laws are rarely evaluated from the perspective of whether they effectively promote women’s interests and rights (Norwitz, Edusa, and Park, 2005). Given that it is women who undergo the processes of treatment, pregnancy and childbirth, it is imperative to consider how reproductive technology legislation affects their well-being.
Regarding factors associated with treatment success, the results indicate that whether the clinic was public or private, and the type of treatment used were two key factors. Women who found that resorting to ARTs represented a minor financial burden (which usually implies greater purchasing power) had higher success rates, probably because of their access to private centres and more advanced treatments. However, when controlling for endogeneity between the characteristics of women accessing ARTs and ARTs success, none of the above variables was found to be significantly associated with treatment success. This may mean that success is ultimately determined by different biological indicators in each organism, which is beyond the control of the present study.
This study has some important methodological limitations. Firstly, it is based on interviews conducted at a single point in time, which precludes capturing events after the time of the survey, especially in the case of young women who may have undergone ARTs at a later point in time. Secondly, since the publication of the data, there have been some important regulatory changes: for example, the public coverage of ARTs has been extended to forty-five years of age in the autonomous community of Madrid. There are also significant differences between autonomous communities in terms of maximum age, number of attempts allowed and requirements according to marital status, which renders a homogeneous interpretation at the national level difficult.
Finally, the small sample size limits the generalisability of the findings, especially in the subgroup of women who reported a need for treatment but economic reasons prevented them from accessing it.
Adserà, Alícia and Lozano, Mariona (2021). “¿Por qué las mujeres no tienen todos los hijos que dicen querer tener?”. Dossier Monográfico: Estado del bienestar, ciclo vital y demografía, 10: 25-33. Observatorio Social, Fundación «la Caixa».
Alcañiz, Mercedes and Monteiro, Rosa (2016). “She-austerity. Precariedad y desigualdad laboral de las mujeres en el sur de Europa”. Convergencia, 72: 39-68.
Alon, Ido; Guimon, José and Urbanos-Garrido, Rosa (2019). “What to Expect from Assisted Reproductive Technologies? Experts’ Forecasts for the Next Two Decades”. Technological Forecasting and Social Change, 148: 119722. doi: 10.1016/j.techfore.2019.119722
Alon, Ido and Pinilla, Jaime (2021). “Assisted Reproduction in Spain: Outcome and Socioeconomic Determinants of Access”. International Journal for Equity in Health, 20: 156. doi: 10.1186/s12939-021-01438-x
Angrist, Joshua D. (1991). Instrumental variables estimation of average treatment effects in econometrics and epidemiology. NBER Working Paper. doi: 10.3386/t0115
Angrist, Joshua D. and Pischke, Jörn-Steffe (2009). Mostly harmless econometrics: An empiricist’s companion. Princeton University Press.
Audibert, Céline and Glass, Daniel (2015). “A Global Perspective on Assisted Reproductive Technology Fertility Treatment: An 8-country Fertility Specialist Survey”. Reproductive Biology and Endocrinology, 13: 133. doi: 10.1186/s12958-015-0131-z
Aurrekoetxea-Casaus, Maite; Ronda, Lorena and Govillard, Leila (2022). “Gender Differences in Attitudes Toward Assisted Reproduction in the Spanish Population: The Weight of Religiosity and Conservatism”. Frontiers in Political Science, 4: 1027997. doi: 10.3389/fpos.2022.1027997
Baranda Ortiz, Aidee (2019). “Factores que interfieren en el incumplimiento de las expectativas reproductivas de las mujeres españolas”. Inguruak, 67: 39. doi: 10.18543/inguruak-67-2019-art03
Billari, Francesco; Goisis, Alice; Liefbroer, Art; Settersten, Richard A; Aassve, Arnie; Hagestad, Gunhild and Spéder, Zsolt (2011). “Social Age Deadlines for the Childbearing of Women and Men”. Human Reproduction, 26(3): 616-622. doi: 10.1093/humrep/deq360
Boivin, Jacky; Bunting, Laura; Collins, John A. and Nygren, Karl G. (2007). “International Estimates of Infertility Prevalence and Treatment-seeking: Potential Need and Demand for Infertility Medical Care”. Human Reproduction, 22(6): 1506-1512. doi: 10.1093/humrep/dem046
Bueno, Xiana (2020). “Fertility Decisions in Transition: Young Adults’ Perceptions on Fertility Three Decades apart in Spain”. The History of the Family, 25(3): 386-405. doi: 10.1080/1081602X.2019.1686049
Castilla, José A.; Hernández, Enrique; Cabello, Yolanda; Navarro, José L.; Hernández, Juana; Gomez, José L.; Pajuelo, Nuria; Marqueta, Javier and Coroleu, Bonaventura (2009). “Assisted Reproductive Technologies in Public and Private Clinics”. Reproductive BioMedicine Online, 19(6): 872-878. doi: 10.1016/j.rbmo.2009.09.028
Chambers, Georgina M.; Hoang, Van Phuong; Sullivan, Elizabeth A.; Chapman, Michael G.; Ishihara, Osamu; Zegers-Hochschild, Fernando; Nygren, Karl G. and Adamson, David G. (2014). “The Impact of Consumer Affordability on Access to Assisted Reproductive Technologies and Embryo Transfer Practices: An International Analysis”. Fertility and Sterility, 101(1): 191-198. doi: 10.1016/j.fertnstert.2013.09.005
Rey, Alberto del; Grande, Rafael and García-Gómez, Jesús (2022). “Transiciones a la maternidad a través de las generaciones: Factores causales del nacimiento del primer hijo en España”. Revista Española de Sociología, 31(2): a108. doi: 10.22325/fes/res.2022.108
Devolder, Daniel and Borisova, Evgeniya (2022). “Demographic Impact of in Vitro Fertilization in Spain”. Medicina Reproductiva y Embriología Clínica, 9(2): 100-115. doi: 10.1016/j.medre.2022.100115
Dhalwani, Nafeesa N.; Fiaschi, Linda; West, Joe and Tata, Laila J. (2013). “Occurrence of Fertility Problems Presenting to Primary Care: Population-level Estimates of Clinical Burden and Socioeconomic Inequalities across the UK”. Human Reproduction, 28(4): 960-968. doi: 10.1093/humrep/des451
Fauser, Bart C. J. M. (2019). “Towards the Global Coverage of a Unified Registry of IVF Outcomes”. Reproductive BioMedicine Online, 38(2): 133-137. doi: 10.1016/j.rbmo.2018.12.001
Fauser, Bart C. J. M.; Boivin, Jacky; Barri, Pedro N.; Tarlatzis, Basil C.; Schmidt, Lone and Levy-Toledano, Rachel (2019). “Beliefs, Attitudes, and Funding of Assisted Reproductive Technology: Public Perception of Over 6,000 Respondents from 6 European Countries”. PLoS ONE, 14(1): e0211150. doi: 10.1371/journal.pone.0211150
Goisis, Alice; Håberg, Siri E.; Hanevik, Hans I.; Magnus, Maria C. and Kravdal, Øystein (2020). “The Demographics of Assisted Reproductive Technology Births in a Nordic Country”. Human Reproduction, 35(6): 1441-1450. doi: 10.1093/humrep/deaa055
Goisis, Alice; Fallesen, Peter; Seiz, Marta; Salazar, Leire; Eremenko, Tatiana and Cozzani, Marco (2024). “Educational Gradients in the Prevalence of MAR Births in a Comparative Perspective”. Fertility and Sterility, 122(4): 648-657. doi: 10.1016/j.fertnstert.2024.05.149
Harris, Katie; Burley, Hugh; McLachlan, Robert; Bowman, Mark; Macaldowie, Alan; Taylor, Kate; Chapman, Michael and Chambers, Georgina M. (2016). “Socio-economic Disparities in Access to Assisted Reproductive Technologies in Australia”. Reproductive BioMedicine Online, 33: 575-584. doi: 10.1016/j.rbmo.2016.07.012
Kocourkova, Jirina; Burcin, Boris and Kucera, Tomas (2014). “Demographic Relevancy of Increased use of Assisted Reproduction in European Countries”. Reproductive Health, 11(1): 37. doi: 10.1186/1742-4755-11-37
Lazzari, Ester; Gray, Edith and Chambers, Georgina M. (2021). “The Contribution of ART to Fertility Rates and Parity Transition: An Analysis of Australian Data”. Demographic Research, 45(34): 1081-1096. doi: 10.4054/DemRes.2021.45.35
Lazzari, Ester; Baffour, Bernard and Chambers, Georgina M. (2022). “Residential Proximity to a Fertility clinic is Independently Associated with Likelihood of Women Having ART and IUI Treatment”. Human Reproduction, 37(11): 2662-2671. doi: 10.1093/humrep/deac205
López-Rodríguez, Silvia (2017). “Políticas públicas y producción de espacios de vulnerabilidad: La construcción de la mujer-madre en el discurso político en España”. Revista Española de Ciencia Política, 44: 97-120. doi: 10.21308/recp.44.04
Martínez-Martínez, Antonio Luis and Bote, Marcos (2019). “Concilia o revienta: Determinantes socioeconómicos y demográficos del uso de técnicas de reproducción humana asistida en perspectiva territorial”. Política y Sociedad, 56(3): 583-601. doi: 10.5209/poso.60510
McCarthy-Keith, Desirée M.; Schisterman, Enrique F.; Robinson, Randal D.; O’Leary, Kathleen; Lucidi, Richard S. and Armstrong, Alicia Y. (2010). “Will Decreasing Assisted Reproduction Technology Costs Improve Utilization and Outcomes Among Minority Women?”. Fertility and Sterility, 94(7): 2587-2589. doi: 10.1016/j.fertnstert.2010.02.021
Melo-Martin, Inmaculada de (2019). “Assisted Reproductive Technology in Spain: Considering Women’s Interests”. Cambridge Quarterly of Healthcare Ethics, 8(3): 228-235. doi: 10.1017/S0963180109090379
Norwitz, Errol R.; Edusa, Valentine and Park, Joong S. (2005). “Maternal Physiology and Complications of Multiple Pregnancy”. Seminars in Perinatology, 29(5): 338-348. doi: 10.1053/j.semperi.2005.08.002
Olsen, Jens; Küppers-Chinnow, Marion and Spinelli, Antonino (1996). “Seeking Medical Help for Subfecundity: A Study Based upon Surveys in Five European Countries”. Fertility and Sterility, 66(1): 95-100. doi: 10.1016/S0015-0282(16)58393-9
Passet-Wittig, Jasmin and Bujard, Martin (2021). Medically assisted reproduction in developed countries: Overview and societal challenges. In: Schneider, N. F. and Kreyenfeld, M. (eds.). Research handbook on the sociology of the family (pp. 417-438). Edward Elgar Publishing. doi: 10.4337/9781788975544.00042
Präg, Patrick and Mills, Melinda C. (2017). “Cultural determinants Influence Assisted Reproduction Usage in Europe more than Economic and Demographic Factors”. Human Reproduction, 32(11): 2305-2314. doi: 10.1093/humrep/dex298
Rochebrochard, Elise de la and Thonneau, Patrick (2005). “Paternal Age: Are the Risks of Infecundity and Miscarriage Higher when the Man is Aged 40 Years or Over?”. Revue d’Épidémiologie et de Santé Publique, 53(2): 47-55. doi: 10.1016/S0398-7620(05)84767-4
Romero Guadix, Bárbara; Díaz Ríos, Patricia; Prados Mondéjar, Fernando; Hernández, Elisa; Cuevas, Irene; Monzó, Ana; Martín, Berta; Llaneza, Plácido; Casas, Ana B.; Castel, Ana B.; Gaspar, Beatriz; Sanz, Clara; Saiz, Maria J.; Peralta, Sara; Iñarra, Maria J. and Castilla Alcalá, Jose A. (2022). “Influencia de los factores socioeconómicos en el acceso a las técnicas de reproducción asistida”. Medicina Reproductiva y Embriología Clínica, 9(1): 100-111. doi: 10.1016/j.medre.2021.100111
Sobotka, Tomas; Hansen, Martin A.; Jensen, Tina K.; Pedersen, Anette T.; Lutz, Wolfgand and Skakkebæk, Niels E. (2008). “The Contribution of Assisted Reproduction to Completed Fertility: An Analysis of Danish Data”. Population and Development Review, 34(1): 79-101. doi: 10.1111/j.1728-4457.2008.00206.x
Sociedad Española de Fertilidad (2018). Registro Nacional de Actividad - Técnicas de Reproducción Asistida: Informe estadístico de Técnicas de Reproducción Asistida.
Stock, James H. and Yoho, Mothiro (2005). Asymptotic distribution of instrumental variables statistics with many instruments. In: Andrews, D. W. K. and Stock, J. H. (eds.). Identification and inference for econometric models (pp. 109-120). Cambridge University Press.
Suero Garcia, Cristina (2024). The moderating role of women’s educational attainment in shaping fertility behaviours in Spain. Castro Martín, María T. and Martín García, Teresa (dirs.), Madrid: Universidad Carlos III. [Doctoral thesis].
Wooldridge, Jeffrey M. (2002). Econometric analysis of cross section and panel data. MIT Press.
Zegers-Hochschild, Fernando; Adamson, David G.; Dyer, Silke; Racowsky, Catherine; Mouzon, Jacques de; Sokol, Rebecca; Rienzi, Laura; Sunde, Arne; Schmidt, Lone; Cooke, Ian D.; Simpson, Joe L. and Poel, Sheryl van der (2017). “The International Glossary on Infertility and Fertility Care”. Human Reproduction, 32(9): 1786-1801. doi: 10.1016/j.fertnstert.2017.06.005
1 This publication is part of the R&D&I projects PID2023-151383OA-100 and PID2020-117980GB-I00 and grant RYC2021-034487 -I, funded by /MICIU/AEI/10.13039/501100011033 and by the European Union NextGenerationEU/PRTR.
Figure 1. Proportion of women receiving ARTs by birth cohort. Cohorts: 1962-1978
Source: Fertility Survey (2018).
Table 1. General characteristics of women who received ARTs (first column) and of those who had unsuccessfully attempted to achieve a pregnancy and did not receive ARTs (second column). Spain, 2018
|
Used ARTs |
Did not use ARTs |
Significant differences |
|||
|
|
N |
% |
N |
% |
p-value |
|
Education level |
|
|
|
|
|
|
Primary or lower |
73 |
9.22 % |
95 |
15.91 % |
0.000 |
|
Secondary |
227 |
37.27 % |
179 |
42.76 % |
|
|
Tertiary |
510 |
45.48 % |
207 |
41.33 % |
|
|
Average age (at start of ARTs) |
|||||
|
Under 30 years old |
167 |
23.24 % |
|||
|
30-39 years old |
567 |
65.65 % |
|||
|
Over 40 years old |
76 |
11.13 % |
|||
|
Religiosity |
|||||
|
Not religious, not at all or not very religious, |
727 |
89.75 % |
413 |
85.86 % |
0.980 |
|
Fairly or very religious |
83 |
10.25 % |
68 |
14.14 % |
|
|
Place of residence |
|||||
|
Urban |
423 |
57.70 % |
254 |
59.06 % |
0.940 |
|
Intermediate |
254 |
31.08 % |
141 |
27.57 % |
|
|
Rural |
133 |
11.22 % |
86 |
13.37 % |
|
|
Autonomous community of residence |
|||||
|
Andalusia |
87 |
15.76 % |
53 |
18.82 % |
0.341 |
|
Aragon |
23 |
2.31 % |
19 |
2.61 % |
|
|
Asturias |
21 |
1.48 % |
29 |
2.04 % |
|
|
Balearic Islands |
29 |
3.15 % |
16 |
2.82 % |
|
|
Canary Islands |
26 |
3.52 % |
27 |
5.61 % |
|
|
Cantabria |
29 |
1.28 % |
22 |
1.08 % |
|
|
Castile and Leon |
44 |
4.74 % |
29 |
3.92 % |
|
|
Castile-La Mancha |
38 |
3.93 % |
20 |
4.46 % |
|
|
Catalonia |
75 |
16.74 % |
52 |
16.4 % |
|
|
Valencia |
72 |
12.04 % |
36 |
10.93 % |
|
|
Extremadura |
31 |
2.08 % |
19 |
2.31 % |
|
|
Galicia |
45 |
4.17 % |
21 |
5.32 % |
|
|
Madrid |
97 |
18.19 % |
57 |
13.91 % |
|
|
Murcia |
37 |
3.27 % |
14 |
3.51 % |
|
|
Navarre |
75 |
1.75 % |
24 |
1.26 % |
|
|
Basque Country |
49 |
4.85 % |
19 |
3.99 % |
|
|
La Rioja |
26 |
0.62 % |
14 |
0.63 % |
|
|
Ceuta and Melilla |
6 |
0.11 % |
10 |
0.4 % |
|
|
Marital status |
|||||
|
Married |
582 |
80.57 % |
274 |
55.35 % |
0.000 |
|
Cohabiting with a partner |
13 |
1.94 % |
207 |
12.7 % |
|
|
Divorced with a partner |
21 |
3.21 % |
1.81 % |
||
|
Single without a partner |
42 |
6.55 % |
398 |
23.6 % |
|
|
Divorced without a partner |
53 |
7.73 % |
83 |
6.55 % |
|
|
Monthly household income (net) |
|||||
|
Below average |
540 |
66.59 % |
345 |
70.92 % |
0.001 |
|
Above average |
270 |
33.41 % |
136 |
29.08 % |
|
|
Individual monthly income (net) |
|||||
|
Less than 1000 euros per month |
396 |
50.12 % |
328 |
66.46 % |
0.000 |
|
More than 1000 per month |
414 |
49.88 % |
153 |
33.54 % |
|
|
Birth cohort |
|||||
|
1962-1965 |
89 |
10.98 % |
50 |
8.35 % |
0.102 |
|
1966-1969 |
119 |
13.88 % |
65 |
11.2 % |
|
|
1970-1974 |
202 |
23.92 % |
99 |
19.69 % |
|
|
1975-1979 |
235 |
27.9 % |
120 |
24.69 % |
|
|
1980-1984 |
109 |
13.16 % |
|||
|
1985-2000 |
56 |
9.56 % |
|||
|
Number of children at start of ARTs |
|||||
|
Childless |
684 |
84.44 % |
|||
|
One child |
101 |
12.47 % |
|||
|
Two or more children |
25 |
3.09 % |
|||
|
Type of employment (at the time of the survey) |
|||||
|
Unemployed |
327 |
40.37 % |
238 |
49.48 % |
0.051 |
|
Temporary employment |
79 |
9.75 % |
74 |
15.38 % |
|
|
Permanent employment |
404 |
49.88 % |
169 |
35.14 % |
|
|
Total |
810 |
481 |
|||
Percentages weighted according to survey recommendations (available at: https://www.ine.es/dyngs/INEbase/en/operacion.htm?c=Estadistica_Cycid=1254736177006ymenu=metodologiayidp=1254735573002).
Source: Fertility Survey (2018).
Table 1. General characteristics of women who received ARTs (first column) and of those who had unsuccessfully attempted to achieve a pregnancy and did not receive ARTs (second column). Spain, 2018 (Continuation)
Table 2. Groups of categories of reported reasons for not undergoing ARTs (N=481). 2018 Fertility Survey. Women
|
Economic reasons (56.5 %) |
Social Security does not cover it, N=56 |
|
My financial situation does not allow me to do so, N=168 |
|
|
I do not have time, N=48 |
|
|
Health reasons |
Due to health problems, N=59 |
|
I have a physical condition that prevents me from undergoing these treatments, N=23 |
|
|
I think it would cause me a lot of stress and emotional exhaustion, N=63 |
|
|
Emotional reasons (13.3 %) |
I prefer to have children by adopting or surrogacy, N=13 |
|
My partner does not want to, N=34 |
|
|
My religious beliefs do not allow me to do so, N=17 |
Source: Fertility Survey (2018).
Table 3. Reasons why women who received ARTs and did not achieve a pregnancy decided to discontinue treatment (N=283)
|
Reasons |
% |
|
I have broken up with my partner |
9.2 |
|
My financial situation does not allow me to do so |
15.2 |
|
Social Security no longer covers it |
10.6 |
|
Emotional exhaustion, stress or anxiety |
24.0 |
|
My partner no longer wants to continue |
3.9 |
|
Due to adoption, surrogacy or pregnancy |
24.7 |
|
Due to health problems |
12.4 |
|
Total |
100 |
Source: Fertility Survey (2018).
Table 4. Probit regression on the probability of ARTs success by women’s individual characteristics at the time of treatment, type of treatment, duration of treatment and ownership of the clinic
|
Coefficient |
p-value |
Confidence interval (95 %) |
||
|
Primary education or lower |
||||
|
Secondary or tertiary |
0.03 |
0.904 |
-0.52 |
0.59 |
|
Religiosity (Not religious or not very religious) |
||||
|
Fairly or very religious |
0.14 |
0.556 |
-0.33 |
0.62 |
|
Average age while receiving ARTs (under 35) |
||||
|
35 or more |
-0.60 |
0.002 |
-0.97 |
-0.22 |
|
Type of treatment (AI) |
||||
|
IVF |
0.35 |
0.047 |
0.00 |
0.69 |
|
Others |
-0.25 |
0.332 |
-0.76 |
0.26 |
|
Ownership of the centre (Social Security) |
||||
|
Private clinic or both |
0.68 |
0.000 |
0.32 |
1.04 |
|
Financial burden represented by ARTs (it was a substantial burden) |
||||
|
Manageable or not problematic |
0.56 |
0.001 |
0.22 |
0.91 |
|
Duration of treatment (less than 1 year) |
||||
|
1-3 years |
-0.36 |
0.026 |
-0.68 |
-0.04 |
|
Over 3 years |
-0.42 |
0.081 |
-0.88 |
0.05 |
|
Constant |
-0.17 |
0.625 |
-0.87 |
0.52 |
|
N |
810 |
|||
|
R2 |
0.043 |
|||
Source: Fertility Survey (2018).
Table 5. Regression model with instrumental variables of ARTs success by women’s individual characteristics at the time of treatment, type of treatment, duration of treatment and centre ownership
|
Coefficient |
p-value |
Confidence interval (95 %) |
||
|
Primary education or lower |
||||
|
Secondary or tertiary |
0.02 |
0.908 |
-0.35 |
0.39 |
|
Religiosity (Not religious or not very religious) |
||||
|
Fairly or very religious |
0.03 |
0.833 |
-0.29 |
0.36 |
|
Average age while receiving ARTs (under 35) |
||||
|
35 or more |
-0.17 |
0.166 |
-0.41 |
0.07 |
|
Type of treatment (AI) |
||||
|
IVF |
0.23 |
0.628 |
-0.71 |
1.17 |
|
Others |
0.08 |
0.887 |
-0.97 |
1.12 |
|
Ownership of the centre (Social Security) |
||||
|
Private clinic or both |
0.06 |
0.834 |
-0.54 |
0.67 |
|
Financial burden represented by ARTs (it was a substantial burden) |
||||
|
Manageable or not problematic |
0.22 |
0.559 |
-0.51 |
0.94 |
|
Duration of treatment (less than 1 year) |
||||
|
1-3 years |
-0.06 |
0.663 |
-0.31 |
0.20 |
|
Over 3 years |
0.00 |
1.000 |
-0.64 |
0.64 |
|
Constant |
0.03 |
0.985 |
-2.82 |
2.88 |
|
N |
810 |
|||
|
Kleibergen-Paap rk Wald F |
26.39 |
|||
Note: The variables educational level, age and financial burden were instrumentalised with “having a partner at the time of starting treatment”.
Source: Fertility Survey (2018).
RECEPTION: January 15, 2025
REVIEW: April 11, 2025
ACCEPTANCE: July 28, 2025